Pyelonephritis / Renal Calculi
Clinical Station (Urology)
Scenario
You are called to A+E to see Mrs Johnson, a 45-year-old woman, presenting with a 4 day history severe right sided back pain and urinary symptoms. She appears unwell, with temperature spikes starting today and tachycardia on initial observations, you have been asked to see her directly due to the A+E being overran.
Observations
Respiratory rate 21
Oxygen saturation 98% on RA
Heart rate 120 BPM
Blood pressure 150/70 mmHg
Temperature 39.2C
How would you initially assess this patient?
Upon receiving the call to assess the patient, I would take the following steps in an A-E approach and CCrISP triple assessment.
Airway
Assess for any signs of airway obstruction
Breathing
Place patient on 15L non-rebreather mask
Monitor oxygen saturation and respiratory rate
Look for cyanosis or increased work of breathing
Perform focused respiratory examination including trachea, percussion, expansion, and auscultation
Obtain ABG/VBG to look for lactate
Circulation
Assess warmth and perfusion
Monitor blood pressure and heart rate
Perform focused cardiovascular examination including pulse regularity, blood pressure, jugular venous pressure (JVP), heart sounds, and signs of overload
Review urine output and fluid balance
Establish intravenous access
Perform blood tests including FBC, U+Es, LFTs, CRP
Obtain an ECG as tachycardic
Disability
Assess Glasgow Coma Scale (GCS)
Check blood glucose levels
Evaluate pupil responses
Monitor temperature and consider blood cultures if indicated
Exposure
Review limbs for evidence of DVT
Review cannula sites for evidence of cellulitis
Examine abdomen for tenderness / peritonitis
If concerned about the patient's condition state you would initiate SEPSIS SIX and promptly inform a senior colleague for further assessment and management.
What are your potential differential diagnoses for this patient?
For a patient presenting with severe back pain and urinary symptoms like Ms. Johnson, potential differential diagnoses can be categorised into urological, gastrointestinal, vascular and gynaecological aetiologies:
Urological
Pyelonephritis
Urinary tract infection (UTI)
Renal calculi
Cystitis
Ureteral obstruction
Gastrointestinal
Acute appendicitis
Diverticulitis
Pancreatitis / cholecystitis
Vascular
Aortic dissection
Renal artery thrombosis / infarction
Gynaecological
Rupture ectopic / ovarian cyst
Endometriosis
What initial bedside tests and haematological investigations would you order in this patient?
Bedside Tests
ABG or VBG: Assess for acidosis and lactate levels, indicating tissue ischemia.
Urine Dipstick: Quickly assess for signs of urinary tract infection (UTI) or haematuria.
Blood cultures: as likely septic
Blood Tests
FBC: Evaluate for signs of infection (e.g. elevated WCC / CRP)
U&Es: Check for electrolyte abnormalities and acute renal failure
LFTs: Assess liver function particularly as likely to start on IV Abx
CRP: Measure to assess for systemic inflammation and potential sepsis.
Scenario: The patient has radiating loin to groin pain (right sided flank pain to RIF) his dipstick was positive for blood and CRP is 250 with WCC 14. She describes urinary symptoms of frequency, urgency and dysuria starting 5 days ago.
What do you think is going on?
Given the constellation of symptoms and findings, including radiating flank pain, haematuria, elevated inflammatory markers, and urinary symptoms, acute pyelonephritis complicated by renal calculi is the most likely diagnosis.
How would you initially treat this patient in A+E?
For the initial treatment of the patient, following the principles of the Sepsis Six protocol (BUFALO mneumonic), the key steps would include:
B Blood Cultures
U Urine Output
F Fluids
A Abx
L Lactate
O Oxygen
Blood Cultures: Collect blood cultures from two different sites.
Urine Output: Catheterise and monitor urine output
Fluids: Initiating rapid IV fluid resuscitation with crystalloid solution.
Abx: Initiating empiric broad-spectrum antibiotics targeting likely pathogens causing pyelonephritis, such as Escherichia coli.
Lactate: Monitor lactate levels if there are signs of systemic illness or shock.
Oxygen: Administering supplemental oxygen if the patient is hypoxic.
Ensure prompt senior clinical review and admission to hospital for further management.
What further radiological investigation would you order?
CT-KUB
Non-contrast CT of the kidneys, ureter and bladder
Gold Standard for investigation of ureteric stones
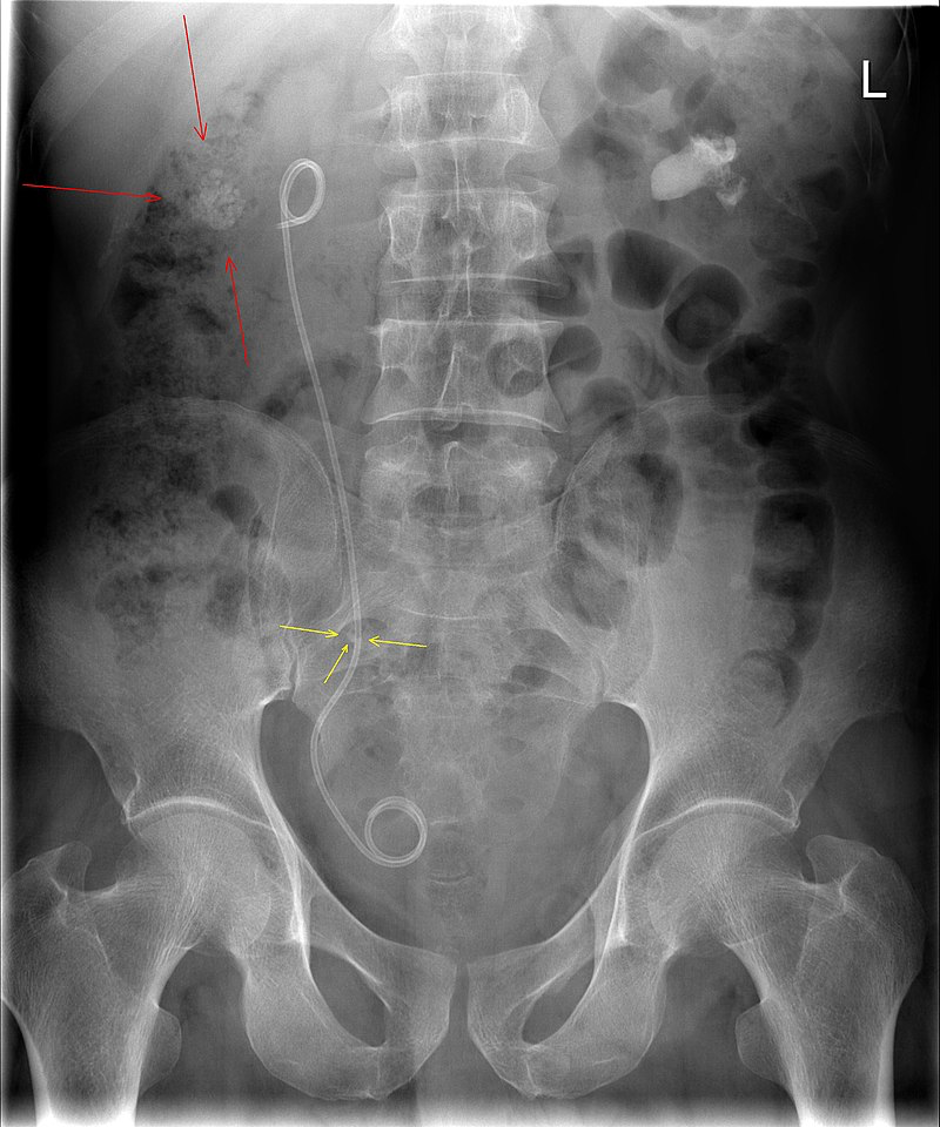
CT KUB shows a right sided 4mm mid-ureteric stone. What further surgical intervention may be required in this patient?
In cases where a patient presents with an infected obstructed urinary system, such as acute pyelonephritis with a ureteric stone, further surgical intervention may be necessary to relieve obstruction and facilitate drainage of infected urine. The two main surgical options in this scenario are nephrostomy tube placement and ureteric stent insertion.
Nephrostomy Tube Placement
Procedure: Tube insertion into renal pelvis through flank.
Indications: Severe ureteric obstruction, infected obstructed system.
Advantages: Rapid relief, direct drainage, bedside procedure.
Disadvantages: Ongoing catheter/tube care, discomfort, risks of bleeding or infection.
Ureteric Stent Insertion
Procedure: Flexible stent placed into ureter.
Indications: Ureteric obstruction, pyelonephritis.
Advantages: Relieves obstruction, minimally invasive.
Disadvantages: Stent-related symptoms, migration, complications.
What is a calculi?
An abnormal solid collection / stone that has precipitated within a duct or organ.
The commonest sites include:
Gallbladder and biliary tree (gallstones)
Urinary system
Pancreas
Prostate
Salivary glands (sialolithiasis)
Where along the renal tract are common sites for stones to become obstructed?
Pelvi-ureteric junction (PUJ)
Pelvic Brim
Vesico-ureteric junction (VUJ)
Note: pelvic brim is where the ureters cross over the iliac vessels
What is the most common composition of renal calculi?
Calcium containing stones. Calcium Oxalate most common
What are the most common organisms for UTI/pyelonephritis?
The three most common causes of urinary tract infections are:
Escherichia coli (E. coli): This bacterium is the most common cause of UTIs, accounting for approximately 80-85% of uncomplicated cases and a significant proportion of pyelonephritis cases.
Klebsiella pneumoniae: Another common Gram-negative bacterium that can cause UTIs, especially in patients with underlying conditions such as diabetes mellitus or structural abnormalities of the urinary tract.
Proteus mirabilis: Known for its ability to form urinary tract stones, Proteus mirabilis is a common cause of complicated UTIs and is frequently associated with urinary catheterisation.
Which infections increase risk of stones? How does this occur?
Proteus
Klebsiella
Mycoplasma
These organisms have the enzyme urease. Urease involved in the hydrolysis of urea. Results in ammonia formation. The resultant alkaline conditions result in the formation of large struvite stones.
Note: Increased pH (alkaline conditions) predisposes to the formation of struvite stones
What are the potential consequences of a renal calculi?
Haematuria
Ongoing renal colic
Obstruction leading to hydronephrosis / hydroureter
Infection
Leading to infected system (pyelonephritis + sepsis)
Malignant transformation
Rare
Squamous cell carcinoma formation
Images